The introduction of monoclonal antibodies has radically changed the field of neuroimmunology and specifically for multiple sclerosis, the monoclonal antibodies targeting B-cells have proven to be very effective therapeutic agents. However, the not uncommon scenario of the co-existence of more than one autoimmune disorder in single patients poses the challenge of attempting to minimize the risks of complications brought on by overlapping multiple immune therapies. The preferable option would be to use one treatment that would combine efficacy across the different diseases. Because randomized clinical trials testing new treatments are not typically designed to investigate effects on patients with two or more immune diseases, case reports provide some evidence-based medicine for clinicians. Here we describe a remarkable clinical improvement observed with two administrations of ublituximab in a 45 year-old male who had juvenile onset of insulin dependent diabetes and had been diagnosed with multiple sclerosis more than ten years earlier. Besides a short course of steroids at the time of diagnosis, the patient had not received any prior disease modifying therapy for multiple sclerosis, and at the time of presentation at our center, he manifested signs and symptoms that led to the new diagnosis of rheumatoid arthritis. With details on the clinical features and laboratory results, this case illustrates the unprecedented attempt to treat the combination of multiple sclerosis and rheumatoid arthritis with ublituximab. An early treatment with a disease modifying therapy capable of a radical impact on the inflammatory activity underlying both multiple sclerosis and rheumatoid arthritis could be viewed as a probable factor for a favorable outcome.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
The field of clinical immunology has been fundamentally transformed by the introduction of treatments based on monoclonal antibodies, not only for their efficacy but also because of the improved understanding of mechanisms underlying immune responses
[1]
Monoclonal antibodies revolutionized biomedical science and health care. Nature 2025, 644, 305.
Chan AC, Martyn GD, Carter PJ. Fifty years of monoclonals: the past, present and future of antibody therapeutics. Nature Reviews Immunology 2025, 25, 745–765.
. This has been the case for multiple sclerosis (MS) where targeting B-cells has unveiled the previously underestimated role of those cells in the autoimmune response and has led to excellent control of the disease
[4]
Hauser SL, Waubant E, Arnold DL, Vollmer T, Antel J, Fox RJ, Bar-Or A. B-cell depletion with rituximab in relapsing-remtting multiple sclerosis. N Engl J Med 2008, 358, 676-688.
Stathopoulos P, Dalakas MC. Role of B cells and pathogenic autoantibodies in autoimmune CNS and PNS neurologic diseases, Handb Clin Neurol. 2026, 214, 47-64.
. However, the coexistence of more than one immune mediated disorder in single patients constitutes a challenge for clinicians. Because clinical trials testing new medications tend to enroll patients without active co-morbidities, class I data on the effects of treatments on accompanying conditions are limited, and decisions can mostly be made on the understanding of the underlying mechanisms driving the disease processes. With the direct consent from the patient, here we report an unprecedented attempt to use ublituximab in a man with pre-existing type I diabetes, untreated MS and newly diagnosed rheumatoid arthritis.
2. Case Report
At 15 years of age, this male patient was diagnosed with type I insulin dependent diabetes. When the patient was 34 year-old he experienced a new onset of impaired sensation to the left leg that within days spread proximally to involve the pelvis as well as the right leg. As the symptoms interfered with the ability to walk, the patient was admitted to the hospital and based on (Magnetic Resonance Imaging) findings, he was diagnosed with MS. After receiving a course of intravenous methylprednisolone, the neurological symptoms resolved and no long-term treatment for MS was initiated. Within two years, a relapse of MS occurred, consisting of sensory disturbances to the left side of the face. Because of the spontaneous recovery within a few days, no treatment was offered. The patient’s mother being affected by systemic lupus erythematosus is viewed as the increased predisposition to autoimmune diseases that this patient carries
[8]
Davidson A, Diamond B. Autoimmune diseases. N Engl J Med 2001, 345, 340-350.
The patient remained under the care of the endocrinologist, treated with insulin for his diabetes, and he continued to function at his usual levels until 44-year-old when he complained of newly developed worsening weakness and muscle wasting. His body weight had gone from 230 lbs to 165 lbs, and because of leg weakness, impaired gait and bladder dysfunction, he was admitted to an outside hospital. The brain and spine documented the presence of demyelinating lesions consistent with MS that, because of the absence of pathological post-contrast enhancements, was thought to be inactive. The patient was discharged with recommendation for long term management by the neurologist as outpatient.
At our initial evaluation, this patient of slender body habitus had intact mentation. He acknowledged diffusely decreased muscle mass and weight loss, significant urinary urgency and difficulties walking due to leg stiffness and weakness. He complained of the impairment of hand dexterity worsening over the previous year impacting his abilities to function at work.
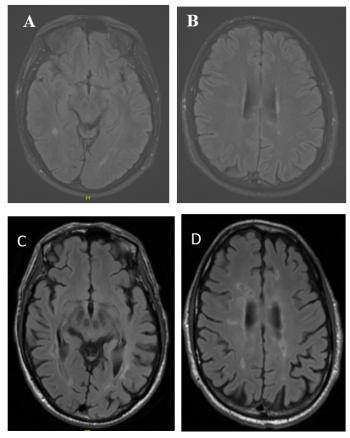
Figure 1. brain at time of MS (A, B) and at time of evaluation at our center (C, D). Examples of T2 Fluid Attenuated Inversion Recovery (FLAIR) sequences demonstrating a few areas of signal abnormalities in the periventricular white matter of the cerebral hemisphere in the initial scans (A, B), progressed and associated with brain volume changes in the more recent scan (C, D).
Cranial nerves were normal with the exception of hearing that was slightly decreased to finger rubs to the left side that patient was aware of. Deformities and diffuse swelling of all the joints of both hands, associated with pain resulted in the inability to clench the hands in a fist. The strength was preserved to the arms, and it was graded at 4 out of 5 to both legs with increased tone and hyperreflexia. The patient had no limb ataxia and sensory testing demonstrated mildly decreased vibratory perception to all four extremities. He complained of aches and pains to the muscles in the thighs and to the knees, and he required arm push to stand up from the seated position. Romberg test was significant for sways with eye closure, and he had a spastic gait with short, cautious strides. Unable to tandem walk, the expanded disability status scale (EDSS) was 4.0; the 9-hole peg test was 19:75 seconds (normal range 10-16 seconds), timed 25-foot walk 6 seconds (normal range 4-5 seconds), symbol digit modality test 48 (normal range 40-60+).
The brain at the time of the MS diagnosis (Figure 1 A, B) showed a few areas of signal abnormalities in the cerebral white matter consistent with an early stage of a demyelinating disease. The brain scan at the time of the evaluation at our center, ten years after the initial images, demonstrated diffuse periventricular and subcortical white matter demyelinating lesions without restricted diffusion or abnormal post-contrast enhancements (Figure 1 C, D). Note was made of the prominent size of the ventricles, basal cisterns and sulci, suggestive of brain volume changes. cervical and thoracic spine, obtained just before the evaluation at our center (images not shown), detected the presence of areas of signal abnormalities consistent with demyelinating lesions related to the diffuse involvement of the spinal cord by MS.
Previously undiagnosed, the patient was found to have positive markers for rheumatoid arthritis, hemoglobin A1c was 6.6%, titers 1:1280 with nucleolar pattern. (Table 1).
Patient initiated treatment with intravenous ublituximab and after two doses six months apart, at the one year follow up, his evaluation was remarkable for the significant improvements of the neurological findings. The patient had resolution of the weakness of the legs and there was a noticeable reduction in the swelling of the joints of the hands that allowed him to regain some of the dexterity of the hands. The EDSS improved to 2.5 (Table 1).
Table 1. Overview of laboratory and clinical parameters.
Patient examinations
Test results pre-treatment
Test results post-treatment
Expanded Disability Status Scale (EDSS)
4.0 (range 0-10)
2.5 (range 0-10)
ANA titers
1:1280 high nuclear, nucleolar pattern
negative
Rheumatoid Factor IgG
<5 units (< = 6 units)
<5 units (< = 6 units)
Rheumatoid Factor IgA
64 units (< = 6 units)
<5 units (< = 6 units)
Rheumatoid Factor IgM
>100 units (< = 6 units)
18 units (< = 6 units)
Cyclic Citrullinated Peptide
>250 units (>59 strong positive)
>250 units (>59 strong positive)
Mutated citrullinated Vimentin antibody
>600 units (<20 units/mL)
Not tested
Complement component C3
132 (nr 82-185 mg/dL)
118 (nr 82-185 mg/dL)
Complement component C4
8 (nr 15-53 mg/dL)
15 (nr 15-53 mg/dL)
3. Discussion
Practicing evidence-based medicine implies endorsing data generated in randomized double-blinded controlled studies but also having insights into the science of the pathophysiology of diseases as well as the mechanisms of action of medications
[9]
Alderazi Y, Bomprezzi R. Are randomized, blind clinical trials enough to guide individualized decisions for patients with neurologic diseases? Neurol Clin Pract 2014, 4(4), 319-328.
. Ublituximab is a newer generation monoclonal antibody designed to target B-cells for depletion and its high efficacy as treatment for MS was established in two phase 3 studies that tested the medication with comparison to oral teriflunomide
[10]
Steinman L, Fox E, M. D., Ph.D., Hartung HP, Alvarez E, Qian P, et al. Ublituximab versus Teriflunomide in Relapsing Multiple Sclerosis. N Engl J Med 2022, 387, 704-714.
Boldrini VO, Mader S, Kumpfel T, Meinl E. Ublituximab: a new FDA-approved anti-CD20 mAb for relapsing forms of multiple sclerosis. Mult Scler Relat Disord 2023, 75, 104733.
At the time of the initial evaluation at our center, the patient whose case is presented here, suffered from three immune mediated diseases, juvenile onset diabetes, MS and the newly diagnosed rheumatoid arthritis. While he had lived with the symptoms of MS for over ten years, the patient got motivated to seek medical attention when the motor impairment of his hands impacted his abilities to work. Patient had not fully recognized that his worsening functional status was contributed to by an undiagnosed rheumatological disorder. The formal scoring for severity of rheumatoid arthritis and an evaluation by the rheumatologist were not pursued. The obvious, diffuse, prominent swelling associated with pain to all the joints of the hands and to the knees were highly suspicious for the disease. The positive markers consistent with an active state of rheumatoid arthritis posed the dilemma of an immune therapy that could treat both of his conditions. B-cell depletion has been a very successful strategy as treatment of MS
[6]
Greenfield A, Hauser S. B cell therapy for multiple sclerosis: entering an era. Ann Neurol. 2018, 83, 13–26.
Boldrini VO, Mader S, Kumpfel T, Meinl E. Ublituximab: a new FDA-approved anti-CD20 mAb for relapsing forms of multiple sclerosis. Mult Scler Relat Disord 2023, 75, 104733.
whereas the response in rheumatoid arthritis could be less predictable due to the diversity of human B-cells and their antibody independent role in immune responses
[14]
Jennifer L Barnas 1, R John Looney 1, Jennifer H Anolik 1 B cell targeted therapies in autoimmune disease. Curr Opin Immunol. 2019, 61, 92–99.
The improvements observed in this patient are worth noting. Given the established efficacy of ublituximab, the silencing of the inflammatory component of MS is not surprising and after two doses of ublituximab, at the one-year assessment, the patient had regained full strength of the legs. Most remarkably, the treatment was associated with lowering of the serum levels of some of the inflammatory markers of rheumatoid arthritis (Table 1) as well as the recovered motor function of the hands. This was significant enough for the patient to be able to return to his manual work as a technician in a manufacturing company.
To our knowledge, this is the first description of the use of ublituximab in a patient suffering from MS and rheumatoid arthritis. Ublituximab exerts its cytolytic effects on the targeted B-cells through antibody- and complement-dependent mechanisms that in this case must have disrupted the duality of the underlying inflammatory response. It is conceivable that the rheumatoid arthritis was at a stage of formation already capable of causing inflammatory reactions to several of the typically affected joints but early enough to be arrested. The change of some of the antibody titers re-tested at one year post-treatment can be interpreted as evidence for the interruption of a disease process still amenable to be modified. However, the persistently elevated cyclic citrullinate peptide antibodies would indicate a disorder demanding continuation of treatment and close monitoring.
In conclusion, our case brings attention to 1) the great efficacy of ublituximab for MS and possibly for rheumatoid arthritis, 2) the opportunity to prioritize treatments with a single agent in patients with coexisting immune-mediated disorders and 3) the better chances for improved outcomes when early interventions are implemented with treatments capable of promptly quieting aberrant autoimmune responses. This latter point lines up with the conceptual advantage of preventing any irreversible tissue damage.
Abbreviations
MS
Multiple Sclerosis
MRI
Magnetic Resonance Imaging
EDSSS
Expanded Disability Status Scale
FLAIR
Fluid Attenuated Inversion Recovery
Acknowledgments
The authors are thankful for the financial support from a private donation by eng. Marco Cherubini.
Author Contributions
Mariana Kurban: Conceptualization, Data curation, Formal analysis, Validation
Chan AC, Martyn GD, Carter PJ. Fifty years of monoclonals: the past, present and future of antibody therapeutics. Nature Reviews Immunology 2025, 25, 745–765.
Hauser SL, Waubant E, Arnold DL, Vollmer T, Antel J, Fox RJ, Bar-Or A. B-cell depletion with rituximab in relapsing-remtting multiple sclerosis. N Engl J Med 2008, 358, 676-688.
Stathopoulos P, Dalakas MC. Role of B cells and pathogenic autoantibodies in autoimmune CNS and PNS neurologic diseases, Handb Clin Neurol. 2026, 214, 47-64.
Alderazi Y, Bomprezzi R. Are randomized, blind clinical trials enough to guide individualized decisions for patients with neurologic diseases? Neurol Clin Pract 2014, 4(4), 319-328.
Steinman L, Fox E, M. D., Ph.D., Hartung HP, Alvarez E, Qian P, et al. Ublituximab versus Teriflunomide in Relapsing Multiple Sclerosis. N Engl J Med 2022, 387, 704-714.
Boldrini VO, Mader S, Kumpfel T, Meinl E. Ublituximab: a new FDA-approved anti-CD20 mAb for relapsing forms of multiple sclerosis. Mult Scler Relat Disord 2023, 75, 104733.
Kurban, M., Morales, I. B., Bomprezzi, R. (2026). Ublituximab Treatment for Multiple Sclerosis and Rheumatoid Arthritis in a Patient with Insulin Dependent Diabetes: A Case Report. Clinical Neurology and Neuroscience, 10(1), 15-19. https://doi.org/10.11648/j.cnn.20261001.13
Kurban, M.; Morales, I. B.; Bomprezzi, R. Ublituximab Treatment for Multiple Sclerosis and Rheumatoid Arthritis in a Patient with Insulin Dependent Diabetes: A Case Report. Clin. Neurol. Neurosci.2026, 10(1), 15-19. doi: 10.11648/j.cnn.20261001.13
Kurban M, Morales IB, Bomprezzi R. Ublituximab Treatment for Multiple Sclerosis and Rheumatoid Arthritis in a Patient with Insulin Dependent Diabetes: A Case Report. Clin Neurol Neurosci. 2026;10(1):15-19. doi: 10.11648/j.cnn.20261001.13
@article{10.11648/j.cnn.20261001.13,
author = {Mariana Kurban and Idanis Berrios Morales and Roberto Bomprezzi},
title = {Ublituximab Treatment for Multiple Sclerosis and Rheumatoid Arthritis in a Patient with Insulin Dependent Diabetes: A Case Report},
journal = {Clinical Neurology and Neuroscience},
volume = {10},
number = {1},
pages = {15-19},
doi = {10.11648/j.cnn.20261001.13},
url = {https://doi.org/10.11648/j.cnn.20261001.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cnn.20261001.13},
abstract = {The introduction of monoclonal antibodies has radically changed the field of neuroimmunology and specifically for multiple sclerosis, the monoclonal antibodies targeting B-cells have proven to be very effective therapeutic agents. However, the not uncommon scenario of the co-existence of more than one autoimmune disorder in single patients poses the challenge of attempting to minimize the risks of complications brought on by overlapping multiple immune therapies. The preferable option would be to use one treatment that would combine efficacy across the different diseases. Because randomized clinical trials testing new treatments are not typically designed to investigate effects on patients with two or more immune diseases, case reports provide some evidence-based medicine for clinicians. Here we describe a remarkable clinical improvement observed with two administrations of ublituximab in a 45 year-old male who had juvenile onset of insulin dependent diabetes and had been diagnosed with multiple sclerosis more than ten years earlier. Besides a short course of steroids at the time of diagnosis, the patient had not received any prior disease modifying therapy for multiple sclerosis, and at the time of presentation at our center, he manifested signs and symptoms that led to the new diagnosis of rheumatoid arthritis. With details on the clinical features and laboratory results, this case illustrates the unprecedented attempt to treat the combination of multiple sclerosis and rheumatoid arthritis with ublituximab. An early treatment with a disease modifying therapy capable of a radical impact on the inflammatory activity underlying both multiple sclerosis and rheumatoid arthritis could be viewed as a probable factor for a favorable outcome.},
year = {2026}
}
TY - JOUR
T1 - Ublituximab Treatment for Multiple Sclerosis and Rheumatoid Arthritis in a Patient with Insulin Dependent Diabetes: A Case Report
AU - Mariana Kurban
AU - Idanis Berrios Morales
AU - Roberto Bomprezzi
Y1 - 2026/03/04
PY - 2026
N1 - https://doi.org/10.11648/j.cnn.20261001.13
DO - 10.11648/j.cnn.20261001.13
T2 - Clinical Neurology and Neuroscience
JF - Clinical Neurology and Neuroscience
JO - Clinical Neurology and Neuroscience
SP - 15
EP - 19
PB - Science Publishing Group
SN - 2578-8930
UR - https://doi.org/10.11648/j.cnn.20261001.13
AB - The introduction of monoclonal antibodies has radically changed the field of neuroimmunology and specifically for multiple sclerosis, the monoclonal antibodies targeting B-cells have proven to be very effective therapeutic agents. However, the not uncommon scenario of the co-existence of more than one autoimmune disorder in single patients poses the challenge of attempting to minimize the risks of complications brought on by overlapping multiple immune therapies. The preferable option would be to use one treatment that would combine efficacy across the different diseases. Because randomized clinical trials testing new treatments are not typically designed to investigate effects on patients with two or more immune diseases, case reports provide some evidence-based medicine for clinicians. Here we describe a remarkable clinical improvement observed with two administrations of ublituximab in a 45 year-old male who had juvenile onset of insulin dependent diabetes and had been diagnosed with multiple sclerosis more than ten years earlier. Besides a short course of steroids at the time of diagnosis, the patient had not received any prior disease modifying therapy for multiple sclerosis, and at the time of presentation at our center, he manifested signs and symptoms that led to the new diagnosis of rheumatoid arthritis. With details on the clinical features and laboratory results, this case illustrates the unprecedented attempt to treat the combination of multiple sclerosis and rheumatoid arthritis with ublituximab. An early treatment with a disease modifying therapy capable of a radical impact on the inflammatory activity underlying both multiple sclerosis and rheumatoid arthritis could be viewed as a probable factor for a favorable outcome.
VL - 10
IS - 1
ER -
Kurban, M., Morales, I. B., Bomprezzi, R. (2026). Ublituximab Treatment for Multiple Sclerosis and Rheumatoid Arthritis in a Patient with Insulin Dependent Diabetes: A Case Report. Clinical Neurology and Neuroscience, 10(1), 15-19. https://doi.org/10.11648/j.cnn.20261001.13
Kurban, M.; Morales, I. B.; Bomprezzi, R. Ublituximab Treatment for Multiple Sclerosis and Rheumatoid Arthritis in a Patient with Insulin Dependent Diabetes: A Case Report. Clin. Neurol. Neurosci.2026, 10(1), 15-19. doi: 10.11648/j.cnn.20261001.13
Kurban M, Morales IB, Bomprezzi R. Ublituximab Treatment for Multiple Sclerosis and Rheumatoid Arthritis in a Patient with Insulin Dependent Diabetes: A Case Report. Clin Neurol Neurosci. 2026;10(1):15-19. doi: 10.11648/j.cnn.20261001.13
@article{10.11648/j.cnn.20261001.13,
author = {Mariana Kurban and Idanis Berrios Morales and Roberto Bomprezzi},
title = {Ublituximab Treatment for Multiple Sclerosis and Rheumatoid Arthritis in a Patient with Insulin Dependent Diabetes: A Case Report},
journal = {Clinical Neurology and Neuroscience},
volume = {10},
number = {1},
pages = {15-19},
doi = {10.11648/j.cnn.20261001.13},
url = {https://doi.org/10.11648/j.cnn.20261001.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cnn.20261001.13},
abstract = {The introduction of monoclonal antibodies has radically changed the field of neuroimmunology and specifically for multiple sclerosis, the monoclonal antibodies targeting B-cells have proven to be very effective therapeutic agents. However, the not uncommon scenario of the co-existence of more than one autoimmune disorder in single patients poses the challenge of attempting to minimize the risks of complications brought on by overlapping multiple immune therapies. The preferable option would be to use one treatment that would combine efficacy across the different diseases. Because randomized clinical trials testing new treatments are not typically designed to investigate effects on patients with two or more immune diseases, case reports provide some evidence-based medicine for clinicians. Here we describe a remarkable clinical improvement observed with two administrations of ublituximab in a 45 year-old male who had juvenile onset of insulin dependent diabetes and had been diagnosed with multiple sclerosis more than ten years earlier. Besides a short course of steroids at the time of diagnosis, the patient had not received any prior disease modifying therapy for multiple sclerosis, and at the time of presentation at our center, he manifested signs and symptoms that led to the new diagnosis of rheumatoid arthritis. With details on the clinical features and laboratory results, this case illustrates the unprecedented attempt to treat the combination of multiple sclerosis and rheumatoid arthritis with ublituximab. An early treatment with a disease modifying therapy capable of a radical impact on the inflammatory activity underlying both multiple sclerosis and rheumatoid arthritis could be viewed as a probable factor for a favorable outcome.},
year = {2026}
}
TY - JOUR
T1 - Ublituximab Treatment for Multiple Sclerosis and Rheumatoid Arthritis in a Patient with Insulin Dependent Diabetes: A Case Report
AU - Mariana Kurban
AU - Idanis Berrios Morales
AU - Roberto Bomprezzi
Y1 - 2026/03/04
PY - 2026
N1 - https://doi.org/10.11648/j.cnn.20261001.13
DO - 10.11648/j.cnn.20261001.13
T2 - Clinical Neurology and Neuroscience
JF - Clinical Neurology and Neuroscience
JO - Clinical Neurology and Neuroscience
SP - 15
EP - 19
PB - Science Publishing Group
SN - 2578-8930
UR - https://doi.org/10.11648/j.cnn.20261001.13
AB - The introduction of monoclonal antibodies has radically changed the field of neuroimmunology and specifically for multiple sclerosis, the monoclonal antibodies targeting B-cells have proven to be very effective therapeutic agents. However, the not uncommon scenario of the co-existence of more than one autoimmune disorder in single patients poses the challenge of attempting to minimize the risks of complications brought on by overlapping multiple immune therapies. The preferable option would be to use one treatment that would combine efficacy across the different diseases. Because randomized clinical trials testing new treatments are not typically designed to investigate effects on patients with two or more immune diseases, case reports provide some evidence-based medicine for clinicians. Here we describe a remarkable clinical improvement observed with two administrations of ublituximab in a 45 year-old male who had juvenile onset of insulin dependent diabetes and had been diagnosed with multiple sclerosis more than ten years earlier. Besides a short course of steroids at the time of diagnosis, the patient had not received any prior disease modifying therapy for multiple sclerosis, and at the time of presentation at our center, he manifested signs and symptoms that led to the new diagnosis of rheumatoid arthritis. With details on the clinical features and laboratory results, this case illustrates the unprecedented attempt to treat the combination of multiple sclerosis and rheumatoid arthritis with ublituximab. An early treatment with a disease modifying therapy capable of a radical impact on the inflammatory activity underlying both multiple sclerosis and rheumatoid arthritis could be viewed as a probable factor for a favorable outcome.
VL - 10
IS - 1
ER -